HIPAA Access Audits for Healthcare Identity Teams 2026
HIPAA Security Rule § 164.312 places identity controls at the center of every covered entity's access-audit risk. OCR enforcement actions have intensified through 2024-25, and the 2026 audit profile is substantively harder than the prior decade. The enterprise reference on the five Technical Safeguards that depend on identity controls, the post-2024 OCR enforcement pattern, and the architecture that produces defensible HIPAA access-audit posture for healthcare IT.

HIPAA Security Rule § 164.312 places identity controls at the center of every covered entity's access-audit risk. OCR enforcement actions have intensified through 2024-25, and the 2026 audit profile is substantively harder than the prior decade. The enterprise reference on the five Technical Safeguards that depend on identity controls, the post-2024 OCR enforcement pattern, and the architecture that produces defensible HIPAA access-audit posture for healthcare IT.
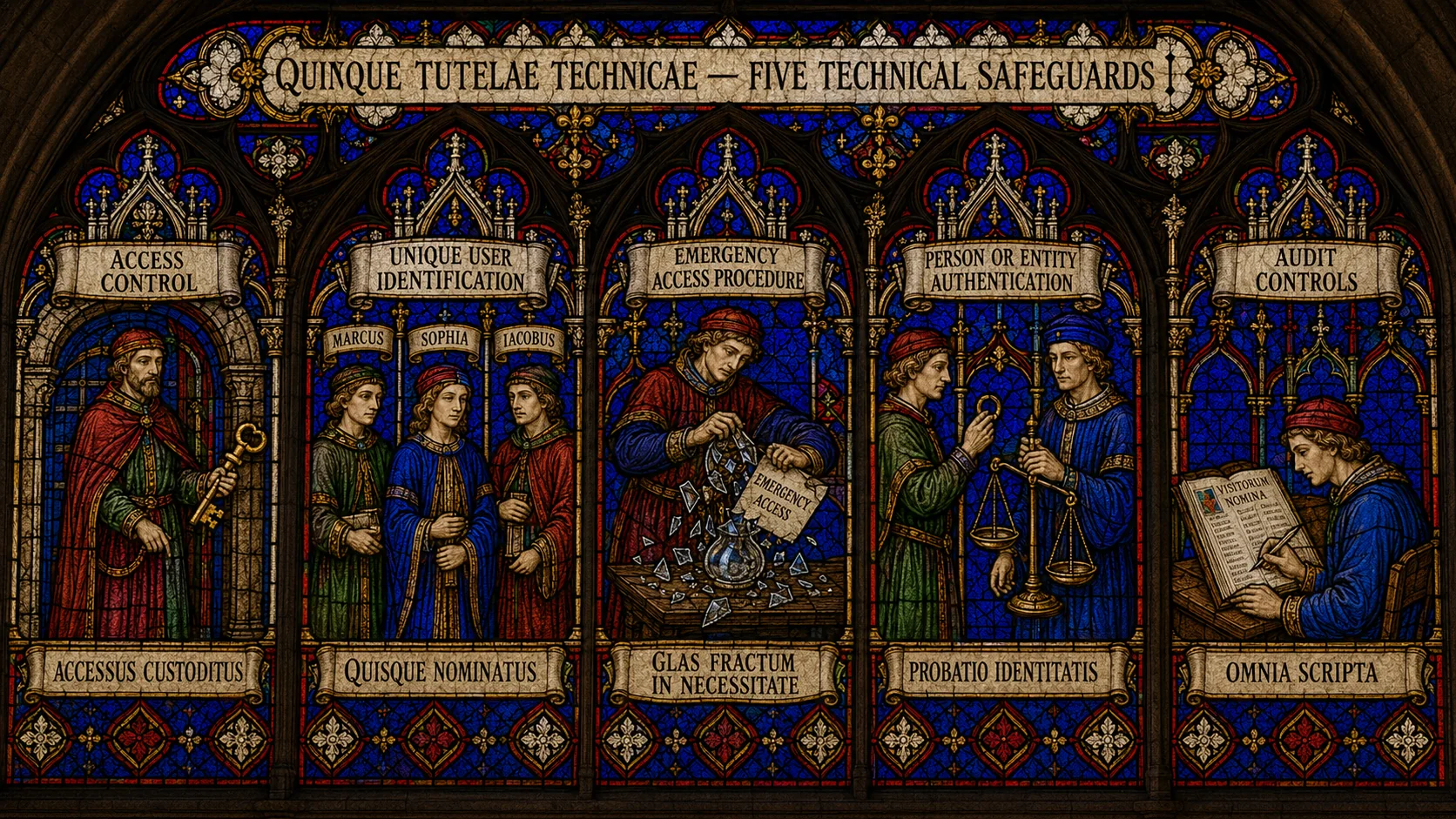
- HIPAA Security Rule § 164.312 (Technical Safeguards) places identity controls at the center of every covered entity's access-audit risk. Five requirements under this section depend directly on the identity architecture: Access Control § 164.312(a)(1), Unique User Identification § 164.312(a)(2)(i), Emergency Access Procedure § 164.312(a)(2)(ii), Person or Entity Authentication § 164.312(d), and Audit Controls § 164.312(b).
- OCR (HHS Office for Civil Rights) enforcement intensified through 2024-25. Resolution agreements doubled in average penalty size compared to 2018-2020. The audit pattern now probes for substantive evidence — not just policy documents but operational data demonstrating that the policies are actually executed.
- Healthcare IAM breaks in four recurring patterns: shared credentials in clinical environments (the nurses-station shared login), persistent emergency access (break-glass that becomes standing access), audit-trail gaps for legacy systems (the 1990s clinical application that doesn't emit SMF-style records), and contractor / temp / locum lifecycle gaps (clinical staff who rotate frequently and produce orphaned access).
- The 2026 reference architecture composes HRIS-driven lifecycle for credentialing-system integration ([HRIS-Driven Lifecycle piece](/en/blog/hris-driven-identity-lifecycle-successfactors-workday-2026/)), strong authentication for clinical workforces including the Identity Challenge Card for deviceless clinical environments ([Phishing-Resistant MFA piece](https://identitychallengecard.avatier.com/en/blog/phishing-resistant-mfa-enterprise-2026/)), structured break-glass procedures with mandatory post-incident review, and SIEM integration that captures the access audit trail across the full healthcare system landscape (EHR + ancillary clinical systems + business systems).
- The architectural test for HIPAA defensibility in 2026 is whether the access audit trail can answer the OCR investigator's question 'who accessed this patient's record on this date and why' in minutes, not days. The post-2024 OCR pattern is to ask this question of specific records during enforcement audits.
HIPAA Security Rule § 164.312 doesn't read like a compliance framework that places identity controls at the center of healthcare IT. The section is titled "Technical Safeguards" and the language is generic enough that on first reading it could apply to almost any access-controlled environment. Section 164.312(a)(1) requires "technical policies and procedures for electronic information systems that maintain electronic protected health information to allow access only to those persons or software programs that have been granted access rights." Sober, technical, abstract. The covered entity's compliance team reads it once and assigns it to IT.
What the section produces operationally is a substantial portfolio of identity-team responsibility. Every clinician access event to a patient's chart. Every shared workstation in the ED. Every break-glass invocation during a code. Every audit log that has to be queryable for a specific patient on a specific date. Every credential issued to a contractor, locum, or temp clinical staff member who rotates through the facility. The HIPAA Security Rule's "Technical Safeguards" section is the foundation of healthcare access-audit risk, and the identity team is the team that builds the foundation.
The 2024-25 OCR enforcement cycle made this real in a way the prior decade hadn't quite. Resolution agreements doubled in average penalty size compared to the 2018-2020 baseline. The audit pattern shifted from "show me the policy" to "show me the audit log for patient X on date Y." Investigators began asking for specific evidence with no notice given to assemble it. The healthcare CISO and the healthcare IT director found themselves in the same audit walkthroughs they'd been preparing for, but with a fundamentally harder evidence bar.
This piece is the 2026 enterprise reference on HIPAA access audits for healthcare identity teams. The five HIPAA Technical Safeguards that depend on identity controls, the post-2024 OCR enforcement pattern, the four recurring patterns that produce healthcare IAM findings, and the integrated architecture that produces continuously defensible HIPAA posture. The companion pieces cover adjacent territory: the SOX Compliance piece covers the financial-system overlap (healthcare organizations with payer relationships often have SOX scope through those relationships), the Access Review piece covers the post-2025 substantive-scrutiny shift relevant across all compliance frameworks, the HRIS-Driven Lifecycle piece covers the credentialing-system integration foundation, the Phishing-Resistant MFA piece on ICC covers the authentication-strength layer including the deviceless Identity Challenge Card for clinical environments, and the PAM piece covers privileged access to clinical systems.
 Five Technical Safeguards, one architecture. Each requirement has operational implications the identity team has to build for and produce evidence of. The architectural test is whether the evidence is generated continuously or assembled at audit time.
Five Technical Safeguards, one architecture. Each requirement has operational implications the identity team has to build for and produce evidence of. The architectural test is whether the evidence is generated continuously or assembled at audit time.
The five HIPAA Technical Safeguards that depend on identity controls
§ 164.312 has five "Required" specifications and three "Addressable" specifications. Five of the eight depend directly on the identity architecture; the other three (Automatic Logoff, Encryption and Decryption, Transmission Security) compose with identity but aren't primarily identity-team responsibilities.
§ 164.312(a)(1) — Access Control (Required). Implement technical policies and procedures that allow access to ePHI only to those persons or software programs that have been granted access rights. This is the umbrella requirement; the rest of § 164.312(a) elaborates how the umbrella is implemented.
The operational implication is that the entitlement model — who can access which ePHI under what conditions — must be documented, enforceable, and auditable. The IGA platform handles the workflow side (who is authorized for what, how access requests flow, how reviews happen); the EHR and ancillary clinical systems handle the enforcement side (what the user can actually do in the system once authenticated). The architectural test is whether the documented entitlement policy and the runtime enforcement actually match — the shadow-provisioning gap documented in our Shadow IT Provisioning piece is exactly the failure mode here.
§ 164.312(a)(2)(i) — Unique User Identification (Required). Assign a unique name and/or number for identifying and tracking user identity.
The operational implication is no shared credentials. No nurses-station shared login. No operating-room kiosk that the surgical team all uses with a common password. No shared workstation in the ED where multiple staff sign in with one identifier. Every ePHI access event in the audit log must attribute to a specific individual.
The clinical-environment reality makes this harder than it sounds. Clinicians move rapidly between workstations during shifts. Logging in fully at each workstation produces operational friction that can affect patient care. The 2026 mature implementation handles this through fast-switch identification (badge tap, smart card, biometric) that lets each clinician authenticate in seconds without compromising the per-user audit trail. The Identity Challenge Card covers the deviceless clinical segment where clinicians can't carry smartphones into sterile environments. The architectural test is whether every ePHI access event attributes to a specific user; events that attribute to a shared identifier produce OCR findings.
§ 164.312(a)(2)(ii) — Emergency Access Procedure (Required). Establish procedures for obtaining necessary ePHI during an emergency.
This is the break-glass requirement. During a clinical emergency — a code, a trauma, a critical patient deteriorating — clinicians need rapid access to patient records that may be outside their normal entitlement scope. The HIPAA requirement is that the covered entity have a procedure for this; the operational reality is that the procedure must work fast enough not to impede patient care AND must produce a full audit trail of the emergency access.
The 2026 mature implementation has four components. Separate credentials (break-glass uses credentials distinct from the user's standard credentials, vaulted in a secure store, requiring explicit checkout). Immediate alerting (the moment break-glass is invoked, security operations is notified through the SIEM). Scoped duration (the session is time-bounded; minutes to hours, never days). Mandatory post-incident review (every invocation requires documented review within a defined window).
The architectural test is whether break-glass invocations show up as exceptional events with full audit trail, or whether break-glass has become the path of least resistance for routine work. The latter is the failure mode that produces OCR findings — break-glass procedures that exist on paper but are operationally indistinguishable from standing access.
§ 164.312(d) — Person or Entity Authentication (Required). Implement procedures to verify that a person seeking access to ePHI is the one claimed.
This is the authentication-strength requirement. Single-factor password authentication is increasingly insufficient for HIPAA-covered ePHI in 2026 — OCR enforcement actions have cited weak authentication as a contributing factor in multiple resolution agreements. The 2026 mature implementation deploys phishing-resistant MFA (passkeys, hardware FIDO2 keys, the Identity Challenge Card for deviceless segments) as documented in our Phishing-Resistant MFA piece on ICC and our Hardware FIDO2 Keys vs Passkeys piece.
The clinical-environment constraint here is that authentication has to be fast enough not to impede patient care. The Identity Challenge Card specifically addresses the deviceless clinical segment — clinicians who can't carry smartphones into sterile environments still need strong authentication that doesn't add 30 seconds to each login.
§ 164.312(b) — Audit Controls (Required). Implement hardware, software, and procedural mechanisms that record and examine activity in information systems that contain or use ePHI.
This is the audit-trail requirement. Every ePHI access — read, write, query, export, print — must be recorded with sufficient detail to support investigation. The audit trail must include the user identity (per § 164.312(a)(2)(i) — uniquely attributed), the patient record accessed, the action taken, and the timestamp.
The operational reality in healthcare is that audit-trail coverage often has gaps. The modern EHR produces robust audit data. The ancillary clinical systems (radiology imaging, lab information systems, pharmacy systems) produce audit data of varying quality. The legacy clinical applications (some still in production from the 1990s) may not produce auditable records at all. The 2026 mature implementation either upgrades, replaces, or wraps the legacy systems with audit-capture middleware — leaving audit gaps is increasingly not OCR-defensible.
SIEM integration is the architectural pattern that composes the audit data from across the system landscape into a queryable corpus. When the OCR investigator asks "show me every access to patient X's record on March 15," the response should be a SIEM query that runs in seconds, not a manual reconstruction across separate system logs.
The post-2024 OCR enforcement pattern
OCR enforcement intensified through 2024-25 in three observable ways. The shift is the audit-side reality that healthcare identity teams now operate under.
Penalty escalation. Resolution agreement penalties roughly doubled in average size compared to the 2018-2020 baseline. The single-largest 2024 settlement set a new high-water mark; subsequent 2024-25 settlements maintained the elevated scale. The signal is that OCR is using its full enforcement authority more aggressively rather than treating most violations as low-tier matters.
Substantive evidence demands. The audit walkthrough has shifted from "show me the policy" to "show me the audit log for patient X on date Y." The change matters because policy documents are usually well-maintained — most healthcare organizations have HIPAA policies that satisfy the audit requirement on paper. Operational audit logs that can answer specific patient-record questions are a different matter; the policy may say the audit log exists, and the audit log may exist in some form, but the ability to query it in minutes for an investigator-named patient is a higher bar.
Access-control focus. The 2024-25 resolution agreements cited access-control breakdowns as contributing factors in many cases. Unauthorized access to ePHI by staff who shouldn't have had the access. Persistent emergency credentials that had become standing access. Shared credentials in clinical environments. Audit-trail gaps for legacy clinical systems. The identity team's domain — exactly the territory § 164.312 covers — is now the most-probed component of an OCR enforcement audit.
The combined effect is that healthcare identity teams now operate under audit conditions where the evidence bar is substantially higher than in prior years and where the consequences of falling short have escalated. The 2026 identity architecture has to produce continuously defensible posture, not policy-defensible posture.
 Same regulatory framework, intensified enforcement. The 2024-25 OCR cycle changed the operational bar for healthcare identity teams substantially. The 2026 architecture has to keep pace.
Same regulatory framework, intensified enforcement. The 2024-25 OCR cycle changed the operational bar for healthcare identity teams substantially. The 2026 architecture has to keep pace.
The four patterns that produce healthcare IAM findings
Four operational patterns recur across 2024-25 OCR resolution agreements and 2026 healthcare identity-team incident reports. Each is operationally addressable; each is also common enough that finding zero examples in a covered-entity environment is rare.
Shared credentials in clinical environments. The nurses-station shared login. The operating-room kiosk. The shared workstation in the ED. The lab terminal that the swing-shift technologists all use with one account. Each pattern violates § 164.312(a)(2)(i) by attributing ePHI access events to a shared identifier instead of a specific individual. The mitigation is fast-switch per-user authentication — badge tap, smart card, biometric — backed by the IDP. The architectural pattern moves the slow per-user login from "30 seconds at every workstation" to "two seconds at every workstation" while preserving the per-user audit trail.
Persistent emergency access. Break-glass procedures that exist on paper but operationally devolve into standing access. The pattern usually starts with one or two clinicians needing rapid emergency access during a code, and over time the break-glass path becomes the easier path for routine work. The audit trail shows break-glass invocations at volumes inconsistent with genuine emergencies. The mitigation is structured break-glass with vault checkout, scoped duration, immediate alerting, and mandatory post-incident review. The volume of break-glass invocations becomes a KPI; sustained elevation triggers investigation.
Audit-trail gaps for legacy systems. The 1990s clinical application that doesn't emit SMF-style records. The radiology imaging system whose audit logs are local-only and aren't aggregated to SIEM. The lab information system whose audit data exists but isn't queryable by patient. When the OCR investigator asks "show me every access to patient X's record on date Y," the gap is the missing system data. The mitigation is system upgrades, replacements, or audit-capture middleware that emits queryable records to the SIEM. Leaving gaps is increasingly not defensible.
Contractor / temp / locum lifecycle gaps. Clinical staff who rotate frequently — locum physicians, traveling nurses, contractor clinical applications staff, residents during their training rotations — produce lifecycle volumes that strain standard joiner-mover-leaver automation. The pattern produces orphaned access (the locum left three weeks ago, but the credentials still work) and over-provisioned access (the contractor was granted broader access than their role required because the manager wanted to avoid having to request more access mid-engagement). The mitigation is HRIS-driven lifecycle that covers all employment classes and the credentialing-system integration that fires deprovisioning the moment privileging expires.
The four patterns are operationally addressable but require deliberate architectural work. Identity teams that haven't focused on these patterns are typically producing OCR-relevant exposure they're not aware of.
The 2026 reference architecture for HIPAA defensibility
The architecture that produces continuously defensible HIPAA posture composes four layers, similar to the SOX architecture but tuned to the healthcare-specific patterns.
Layer 1: HRIS-driven credentialing-system integration. The HRIS handles the workforce-membership authority. The credentialing system (typically a healthcare-specific application like Cactus, Echo, or ProviderTrust) handles the clinical-privileging authority — what specific clinical privileges each clinician holds, when they were granted, when they expire. Both systems feed the IGA platform; the IGA platform produces the integrated access decisions across employment status AND clinical privileging. The HRIS-Driven Lifecycle piece covers the HRIS foundation; the credentialing-system layer is healthcare-specific extension.
Layer 2: Strong authentication for clinical workforces. Phishing-resistant MFA at the workforce baseline. Fast-switch authentication for clinical workstation scenarios where shared workstations are physically necessary. The Identity Challenge Card for deviceless clinical environments where smartphones can't be carried. The Phishing-Resistant MFA piece on ICC and Hardware FIDO2 vs Passkeys piece cover this layer in detail. The architectural test is whether every clinician can authenticate strongly in their actual workflow context — clinical environments have constraints that retail or office environments don't.
Layer 3: Structured break-glass with audit-trail completeness. Break-glass credentials are vaulted, separate from standing credentials, time-bounded, immediately alerted. Post-incident review is mandatory within a defined window. Volume metrics are tracked and elevated invocations trigger investigation. The architectural test is whether break-glass invocations look like exceptional events in the audit data or whether they look like routine access.
Layer 4: SIEM-integrated audit trail across the full healthcare system landscape. Every ePHI-touching system emits audit records to a central SIEM. Query infrastructure can answer the OCR investigator's specific-patient question in minutes. Legacy systems either emit native audit records, are wrapped with audit-capture middleware, or are slated for replacement. Audit-trail gaps are documented (not hidden) and tracked toward remediation.
The four layers compose into continuously defensible posture — the architectural goal post-2024 OCR enforcement intensified the audit-cycle expectations.
The 2026 reference path
Map every clinical and business system that touches ePHI to the five Technical Safeguards. Confirm access control is enforced, unique user identification is attributed, emergency access has structured procedure, authentication is strong, audit controls are queryable. Systems where any of the five fails are exposure surface.
Address the four recurring failure patterns explicitly. Shared credentials in clinical environments — deploy fast-switch authentication. Persistent emergency access — restructure break-glass with vault checkout and mandatory review. Audit-trail gaps — upgrade, replace, or wrap legacy systems with audit-capture middleware. Contractor / locum / temp lifecycle — extend HRIS-driven automation to cover all employment classes.
Compose the four-layer architecture. HRIS + credentialing-system integration for the lifecycle foundation. Strong authentication including Identity Challenge Card for deviceless clinical segments. Structured break-glass with audit completeness. SIEM-integrated audit trail across the full healthcare landscape.
Test the architecture against the OCR-question standard. "Show me every access to patient X's record on date Y" should be answerable in minutes. Run the query against your own audit trail periodically; if the answer takes hours or has gaps, the architecture isn't OCR-ready yet.
Compose with the broader compliance stack. The SOX Compliance piece covers the financial-system overlap (most healthcare organizations have SOX scope through payer relationships). The Access Review piece covers the substantive-scrutiny shift that applies across compliance frameworks. The Shadow IT Provisioning piece covers the catalog-reality gap that produces both SOX and HIPAA findings. The ISPM piece covers the continuous-posture layer that makes the defense continuous.
HIPAA enforcement intensified meaningfully in 2024-25. The audit-cycle expectations of 2026 are substantively harder than the prior decade. Healthcare identity teams whose architecture kept pace are still passing OCR walkthroughs cleanly. Healthcare identity teams whose architecture stayed in the prior pattern are producing findings that wouldn't have surfaced before. The path forward is the continuously-defensible architecture this piece describes — make the transition deliberately.
ABOUT THE AUTHOR

More from Compliance & Audit
SOX Compliance for Identity Teams 2026: What Auditors Actually Want to See
Sarbanes-Oxley Section 404 places IT general controls (ITGC) over financial systems squarely in the IAM team's lap — even though SOX itself doesn't mention identity once. The 2026 enterprise reference on the five SOX ITGC domains that depend on identity controls, the auditor expectations that shifted in the post-2025 audit cycle, and the architecture that produces clean SOX walkthroughs.
The Access Review Your Auditor Actually Wants 2026
Most enterprise access reviews are checkbox exercises — manager attests, audit log records, cycle closes. The auditor walks away with a binder of attestation evidence and the program reports clean. The 2026 auditor profile asks harder questions: did the reviewer actually engage, does the catalog match target-system reality, and what changed as a result. The enterprise reference on the three questions auditors actually ask now and the five review patterns that pass the test.
The Real Cost of a Help Desk Password Reset (It's Not $15) 2026
The $15-per-password-reset figure that's been quoted for two decades undercounts the true cost meaningfully. The 2026 enterprise reference on the five cost components that make up the actual per-reset price, why each one undercounts, how to compute the number for your own organization, and the savings model when reset automation is deployed properly.